

hepatic steatosis
- douglasrodrigomatt

- Jun 25, 2025
- 5 min read
This post was automatically translated into English by ChatGPT. Please consider occasional grammatical errors during your reading and interpretation. Happy studying! Several organs can be affected by fatty infiltration, but the liver is particularly a common target of this condition, mainly due to its metabolic functions. Therefore, knowing how to identify hepatic steatosis is important, and beyond that, knowing how to grade and understand the severity of this often underestimated finding.
why does it happen?
There are several causes of fat accumulation in hepatocytes, the vast majority being metabolic in origin. Patients with diabetes mellitus, hypercortisolism, and hypothyroidism often develop hepatic fat accumulation as a consequence of these conditions. In each of these conditions, the pathophysiology by which this occurs is different, but the common result is the same: chronic fat deposition in the liver.
Just like in hypercortisolism (due to increased systemic cortisol), patients using corticosteroids may also develop hepatic steatosis.
In addition, chronic inflammation in other organs (such as the pancreas and intestines) alters metabolism and, unsurprisingly, leads to hepatic fat deposition.Oh, and let's not forget the breeds that are predisposed to these diseases: Schnauzers? They love to develop diabetes mellitus and hypercortisolism. Hypercortisolism? Keep an eye on shih tzus, lhasas, malteses, dachshunds, poodles... anyway, the list is long, right?
in the image
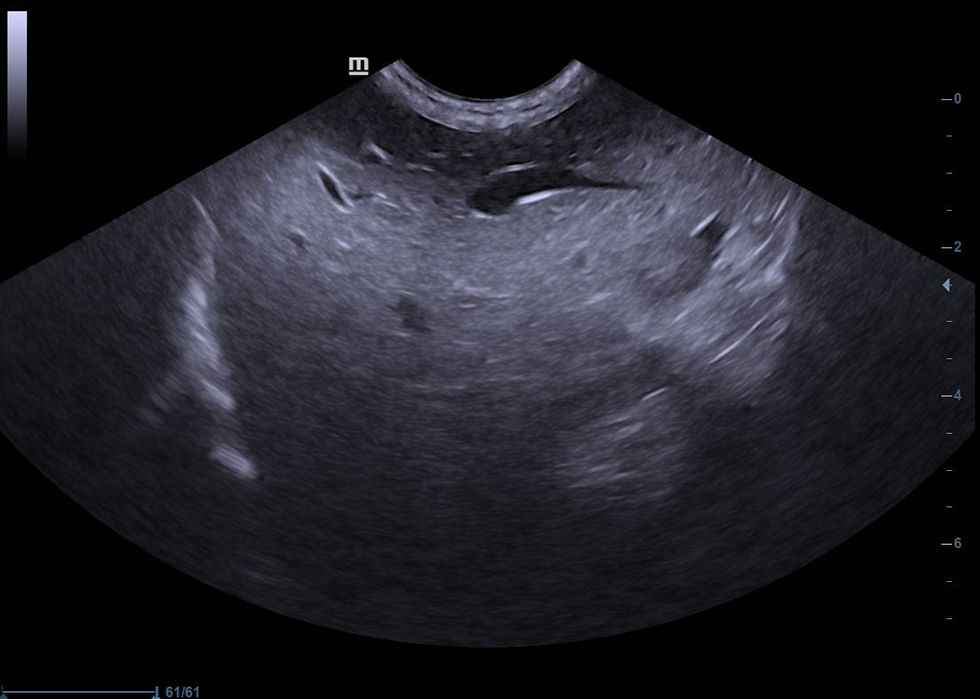
Ultrasonographically, the main characteristic finding of hepatic steatosis is increased echogenicity of the parenchyma, associated with posterior beam attenuation. This occurs because fat is much more echogenic than the liver parenchyma, reflecting the sound waves (making the parenchyma appear more echogenic) and not allowing the waves to penetrate into the deeper portions of the tissue (promoting attenuation of the beams). This hyperechogenicity can be similar to that of falciform fat, greater than it, or even less echogenic than the falciform fat.
It is common for this parenchyma to appear slightly more coarse than normal, as a result of fibrotic areas interspersed within the tissue (which we will understand later).
Another hepatic parameter altered in these cases is the size and contour of the liver. Fat takes up more space than healthy hepatocytes, so the liver parenchyma tends to enlarge (variable hepatomegaly) and the liver borders become bulging (or rounded).
As the parenchyma increases in size and stiffness, it begins to compress the vessels, making especially the hepatic veins more difficult to visualize (pay attention to this information).
importance of diagnosis
It is essential to promptly identify hepatic steatosis because measures must be taken by the clinician or gastroenterologist, as hepatic fat causes chronic inflammation in the parenchyma, and as this parenchyma begins to suffer, hepatocytes are replaced by fibrous tissue (hence the coarse appearance). Furthermore, it has been studied that in humans, rats, and our canine patients, this fatty infiltration leading to chronic inflammation precedes hepatic neoplasia (hepatocarcinoma). In other words, if this patient remains with hepatic steatosis, they presumably have two possible outcomes: chronic inflammation that may progress to hepatic cirrhosis, or chronic inflammation that may progress to hepatocarcinoma.
Therefore, fatty infiltration should be studied at a histopathological level to determine the stage of the condition's pathophysiology.
In addition, ultrasonographically, this lesion must be graded.
grading of hepatic steatosis
Grading is important since this is a chronic condition, and the patient will need monitoring. Staging is essential for treatment protocols to be adjusted over time. Grading can be subjective (B-mode) or objective (Doppler study).
subjective grading – B-mode
In B-mode, we can study the degree of beam attenuation intensity and its effect on the definition of the diaphragmatic line. For this, we direct the sound beam in a longitudinal plane via the right paracostal approach, visualizing the gallbladder and the diaphragmatic line, and based on that, we perform our grading of hepatic steatosis as follows:
mild (grade I): attenuation of sound beams is observed, with no effect on the definition of the diaphragmatic line
moderate (grade II): beam attenuation begins to also cause attenuation of the diaphragmatic line image
severe (grade III): beam attenuation causes obliteration, meaning: loss of definition of the diaphragmatic line

Always pay close attention to the machine settings, such as focus and TGC, when evaluating a liver suspected of fatty infiltration.
qualitative grading – pulsed Doppler
Basically, in a similar imaging plane to the one previously mentioned, we can observe the hepatic vein, which is the last abdominal vein to anastomose with the vena cava before it reaches the right atrium. Precisely because of this, the right hepatic vein is directly influenced by the changes in red blood cell velocity secondary to the right cardiac cycle. These velocity changes can be observed in the hepatic vein using pulsed Doppler, and are only possible thanks to the compliance (softness) of healthy liver tissue. As this hepatic tissue becomes rigid, it allows less compliance of the hepatic vein and less variation in flow velocity during each phase of the cardiac cycle.
We know that as fatty infiltration progresses, liver parenchyma stiffness increases (due to the fat itself and secondary fibrosis from chronic inflammation). Therefore, the more altered the waveform morphology of the hepatic vein, the more rigid the parenchyma is, and the more severe the liver lesion becomes.
Thus, based on the waveform morphology of the right hepatic vein, we can grade hepatic steatosis as follows:
mild (grade I): when fatty infiltration is seen in B-mode, but the hepatic vein shows no waveform morphology changes (i.e., the steatosis is mild and not enough to alter the vein’s compliance)
moderate (grade II): when the hepatic vein displays a monophasic waveform, but still with some oscillations
severe (grade III): when the waveform remains monophasic but without oscillations, exhibiting a pattern referred to as portalized.

It’s worth noting that the higher the degree of fatty infiltration, the more compressed the hepatic vein becomes—making it more difficult to locate and evaluate with Doppler.
We classify it as a subjective and a qualitative grading because in B-mode, technical settings and the individual “eye” of each ultrasonographer may interpret the image differently, whereas the waveform morphology in pulsed Doppler is consistently interpreted regardless of the observer.
a generally chronic condition, but...
We must remember that an equally hyperechoic image with posterior beam attenuation (also ultrasonographically classified as fatty infiltration) is hepatic lipidosis, which has a completely different pathophysiology.More common in overweight or obese patients (especially those who already had hepatic steatosis), but not exclusive to them, it is diagnosed in those with prolonged anorexia, where the demand for energy through neoglucogenesis results in the breakdown of fat stored in tissues. This overwhelms the liver with more fat than it can metabolize, so it stores it (in this case, acutely), which may lead to hepatic failure.
other evaluation methods
There are other ways to assess hepatic steatosis in our patients, such as histogram analysis and elastography.
As supplementary material, we have a recent (and national) article about histogram use in evaluating fatty infiltration — definitely worth a read.
As for elastography, the concept is simpler. Elastography can assess the softness or stiffness of the tissue, and as we've seen throughout the post, fatty infiltration (and subsequent fibrosis) makes the parenchyma stiffer. Thus, elastography can be very effective in this evaluation.However, I leave here my personal remark: the position beneath the rib cage, where the liver lies, significantly limits the use of compression elastography, making this technique difficult to apply. Furthermore, this technique compares different tissue consistencies within a specific sample volume — meaning that to know if a tissue is “stiffer,” the same sample must include a portion of healthy tissue as a reference. Since fatty infiltration generally affects the entire liver, it becomes very difficult to obtain truly diagnostic information using compression elastography.
On the other hand, shear wave elastography, in which the device itself generates the shear wave and provides numerical data on tissue stiffness, does provide diagnostic information, since normal reference values are already established for each organ and species.
Comments